



Nine Muscle Myths That Keep Mid-Life Adults Weak
Post 6 of 7 · Countdown to World Sarcopenia Day (4 July 2025)
Christine, 68, came to clinic convinced her weakness was “just aging.” She had lost 12 lb since 2022 yet struggled to lift a suitcase overhead.
Grip strength 14 kg (cut-off < 16 kg for women)
Five-sit-to-stand 18 s (goal ≤ 15 s)
Protein 0.7 g·kg⁻¹ — not even the RDA
Her story mirrors hundreds I see in clinic and consults. Most patients arrive carrying the same myths that quietly erode muscle, power, and independence

.
Why Busting Myths Matters
Low lean mass predicts slower gait, higher fall risk, longer hospital stays, and roughly double all-cause mortality. Encouragingly, about 70 percent of late-life strength is shaped by modifiable factors such as activity and nutrition rather than calendar age².
The Nine Myths
Myth 1 “It’s just aging.”
Lifestyle drives much of the decline; progressive resistance training can restore nearly 10 percent of thigh-muscle area in older adults, even those in their eighties, within 8–12 weeks²³.
Myth 2 “Older adults need less protein.”
Because of anabolic resistance, adults over 65 may benefit from 1.2–1.6 g·kg⁻¹·day⁻¹ protein to maintain muscle mass⁴. In a 12-week study, spreading protein evenly across meals added 1.5 kg lean mass versus 0.8 kg with a skewed pattern⁵.
Myth 3 “Strength training is dangerous after 60.”
Meta-analyses show supervised lifting in adults 60 + increases strength by 30–40 percent with injury rates comparable to walking programs⁶.
Myth 4 “Muscle turns to fat if you stop lifting.”
Muscle and fat are biologically distinct tissues; muscle loss and fat gain can co-occur during inactivity, but one does not “turn into” the other⁷.
Myth 5 “You can’t build muscle over 70.”
Adults in their eighties gained ~1.5 kg lean mass and > 100 percent leg strength in just eight weeks of progressive resistance training³.
Myth 6 “No weight loss means no progress.”
Pairing resistance exercise with a higher-protein diet helped older adults preserve lean mass and improve body composition despite only modest weight change⁸.
Myth 7 “You need an hour in the gym.”
In sedentary men, shorter aerobic sessions produced fat loss similar to longer ones; strength was not assessed in that trial⁹.
Myth 8 “Only 8–12 reps build muscle.”
High-rep, low-load sets (25–35 reps) can match traditional 8–12-rep hypertrophy if sets are pushed near failure¹⁰.
Myth 9 “You must eat protein right after lifting.”
Total daily protein drives muscle growth more than strict timing; evidence indicates the anabolic window spans several hours post-exercise¹¹.
Screen • Train • Fuel
Problem
Nearly half of adults over 60 still eat ≤ 0.8 g·kg⁻¹ protein while lifting⁴, forfeiting about 25 percent of potential lean-mass gain.
Screen
SARC-F ≥ 4, grip < 27 kg (men) or < 16 kg (women), or five-sit-to-stand > 15 s → start today
Track three typical eating days
Train
Two full-body resistance sessions each week
Week 1 at RPE 5, progressing to RPE 7–8 by Week 4
Include one power move (loaded carries or medicine-ball throws)
Fuel
Protein targets
Healthy adults ≥ 1.2 g·kg⁻¹·day⁻¹
Weakness or sarcopenia 1.2–1.6 g·kg⁻¹·day⁻¹
Aim for three meals of ~30 g protein; daily total is the priority
Next-Level Add-Ons
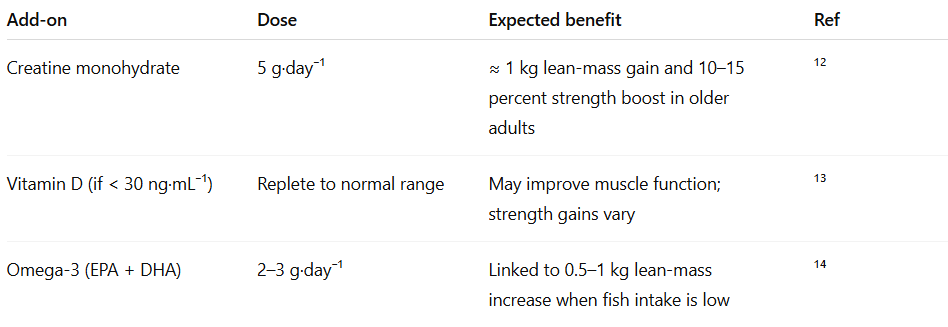
Lock training and protein first; supplements enhance but never replace fundamentals.
Christine’s Turnaround
Christine applied Screen • Train • Fuel:
Protein raised to 1.3 g·kg⁻¹
Two 30-minute lifting sessions per week
Ten-minute loaded carry daily
Six months later she added 1.3 kg lean mass, cut sit-to-stand to 12 s, and hiked the Blue Ridge in May. Aging was not the culprit; misinformation was.
Share Your Take
Have you noticed muscle changes after forty?
Save this for your next clinic visit or workout and share with someone still clinging to these myths.
Be sure to subscribe so you get each post delivered to your email.
References
Dhillon RJ, Hasni S. Pathogenesis and management of sarcopenia. Clin Geriatr Med. 2017;33(1):17-26. doi:10.1016/j.cger.2016.09.003
Zempo H, Kimura T, Onambélé GL, et al. Heritability estimates of muscle strength–related phenotypes: a systematic review and meta-analysis. Age (Dordr). 2017;39(1):8. doi:10.1007/s11357-017-9958-1
Fiatarone MA, Marks EC, Ryan ND, Meredith CN, Lipsitz LA, Evans WJ. High-intensity strength training in nonagenarians: effects on skeletal muscle. JAMA. 1990;263(22):3029-3034. doi:10.1001/jama.1990.03440220053029
Traylor DA, Gorissen SHM, Phillips SM. Perspective: protein requirements and optimal intakes in aging: are we ready to recommend more than the RDA? Adv Nutr. 2018;9(3):171-182. doi:10.1093/advances/nmy019
Yasuda J, Tomita T, Arimitsu T, Fujita S. Evenly distributed protein intake over three meals augments resistance exercise–induced muscle hypertrophy in healthy young men. J Nutr. 2020;150(7):1845-1851. doi:10.1093/jn/nxaa101
Fragala MS, Cadore EL, Dorgo S, et al. Resistance training for older adults: position statement from the National Strength and Conditioning Association. J Strength Cond Res. 2019;33(8):2019-2052. doi:10.1519/JSC.0000000000003231
Goodpaster BH, Carlson CL, Visser M, et al. Attenuation of skeletal muscle and strength in the elderly: effect of functional limitations and physical activity. J Gerontol A Biol Sci Med Sci. 2001;56(10):B449-B455. doi:10.1093/gerona/56.10.B449
Verreijen AM, Engberink MF, Houston DK, et al. Dietary protein intake and weight-loss–induced muscle mass loss in older adults. J Nutr Health Aging. 2015;19(7):741-748. doi:10.1007/s12603-015-0503-7
Rosenkilde M, Auerbach PL, Reichkendler MH, et al. Body-fat loss and compensatory mechanisms with different doses of aerobic exercise: a randomized trial in overweight sedentary men. Am J Physiol Regul Integr Comp Physiol. 2012;303(6):R571-R579. doi:10.1152/ajpregu.00128.2012
Schoenfeld BJ, Peterson MD, Ogborn D, Contreras B, Sonmez GT. Effects of low- versus high-load resistance training on muscle strength and hypertrophy in well-trained men. J Strength Cond Res. 2015;29(10):2954-2963. doi:10.1519/JSC.0000000000000958
Schoenfeld BJ, Aragon AA, Krieger JW. The effect of protein timing on muscle strength and hypertrophy: a meta-analysis. J Int Soc Sports Nutr. 2013;10(1):53. doi:10.1186/1550-2783-10-53
Candow DG, Forbes SC, Chilibeck PD, et al. Effects of creatine supplementation and resistance training on muscle mass and muscle function in older adults: a meta-analysis. Nutrients. 2019;11(8):1861. doi:10.3390/nu11081861
Ceglia L. Vitamin D and its role in skeletal muscle. Curr Opin Clin Nutr Metab Care. 2009;12(6):628-633. doi:10.1097/MCO.0b013e328331c707
Smith GI, Atherton P, Reeds DN, et al. Omega-3 polyunsaturated fatty acids augment resistance exercise training–induced increases in muscle mass and strength in older adults. Am J Clin Nutr. 2011;93(2):402-412. doi:10.3945/ajcn.110.005611
Although I can only offer a p=1, adding MSM to my daily regime has helped.
Current dosage is 4mg daily; I found larger doses (...maybe due to when they were taken...?) caused mild stomach distress. Has improved joint comfort as well as helping with age-related skin issues.
Found these on a cursory search; some of them aren't specifically addressing aged population but they do give a decent overview of the benefits:
https://pmc.ncbi.nlm.nih.gov/articles/PMC5521097/
Effects of Methylsulfonylmethane (MSM) on exercise-induced oxidative stress,
muscle damage, and pain following a half-marathon: a double-blind, randomized,
placebo-controlled trial
https://www.sciencedirect.com/science/article/pii/S1756464623004383?via%3Dihub
The effect of a 12-week dietary intake of food supplements containing collagen
and MSM on dermis density and other skin parameters: A double-blind,
placebo-controlled, randomised four-way study comparing the efficacy of three test products
https://pmc.ncbi.nlm.nih.gov/articles/PMC4502733/
Evaluation of the Effect of Mega MSM on Improving Joint Function in
Populations Experiencing Joint Degeneration
https://www.sciencedirect.com/science/article/pii/S1063458405002852
Efficacy of methylsulfonylmethane (MSM) in osteoarthritis pain of the knee: a pilot clinical trial1,2
Appreciate all you do!